ADHD DSM-5 Criteria – Symptoms, Presentations, and Diagnosis Explained
If you've been researching ADHD, you may have come across references to the ADHD DSM-5 criteria — the clinical standard that healthcare professionals rely on to identify attention-deficit/hyperactivity disorder. However, clinical language can feel dense and hard to apply to your own life. Whether you're exploring these criteria for yourself or for someone you care about, a free ADHD self-reflection quiz can help you organize your thoughts. This guide breaks down every DSM-5 criterion for ADHD in plain language. You'll find the full symptom checklists, the three ADHD presentations, how the criteria differ for adults, what the diagnostic codes mean, and what changed from previous editions. By the end, you'll understand exactly what the DSM-5 says about ADHD.
What Is ADHD According to the DSM-5?
ADHD stands for attention-deficit/hyperactivity disorder. The DSM-5 — short for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition — is published by the American Psychiatric Association. It serves as the primary reference guide that clinicians use to evaluate and diagnose mental health conditions, including ADHD.
Under the DSM-5, ADHD is classified as a neurodevelopmental disorder. This means it originates during the developmental period and involves difficulties in personal, social, academic, or occupational functioning. The DSM-5 describes ADHD as a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development.
Why does this framework matter? Because the DSM-5 criteria create a shared, evidence-based language for diagnosis. Without standardized criteria, recognizing ADHD would depend entirely on subjective judgment. The DSM-5 helps ensure that whether you visit a psychiatrist in New York or a psychologist in London, the same foundational standards inform the evaluation process.
Complete DSM-5 Symptom Criteria for ADHD
The ADHD DSM-5 criteria include two main categories of symptoms: inattention and hyperactivity-impulsivity. Each category lists nine specific symptoms. For a diagnosis, children up to age 16 must show at least six symptoms in one or both categories. Adolescents aged 17 and older and adults need at least five.
These symptoms must have persisted for at least six months, and they must be inconsistent with what's developmentally appropriate.
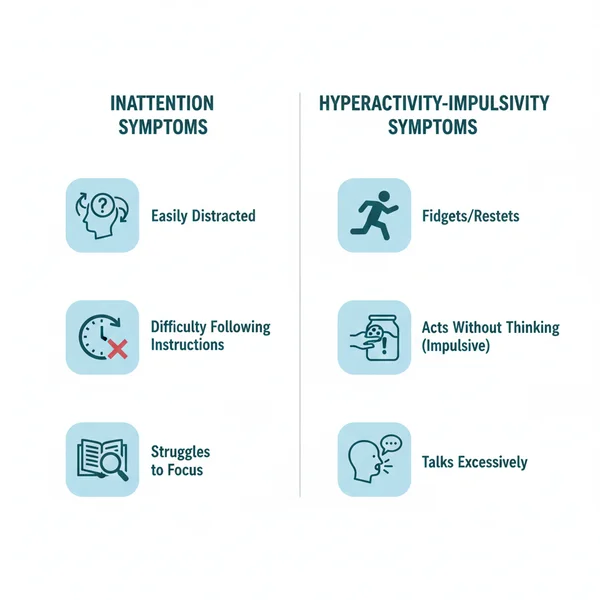
9 Inattention Symptoms in the DSM-5
According to the DSM-5 criteria for ADHD, the inattention symptoms are:
- Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities.
- Often has trouble holding attention on tasks or play activities.
- Often does not seem to listen when spoken to directly.
- Often does not follow through on instructions and fails to finish schoolwork, chores, or workplace duties.
- Often has trouble organizing tasks and activities.
- Often avoids, dislikes, or is reluctant to do tasks that require sustained mental effort over a long period.
- Often loses things necessary for tasks and activities — such as keys, paperwork, glasses, or mobile phones.
- Is often easily distracted by unrelated thoughts or stimuli.
- Is often forgetful in daily activities.
9 Hyperactivity-Impulsivity Symptoms in the DSM-5
The DSM-5 also lists these hyperactivity and impulsivity symptoms:
- Often fidgets with or taps hands or feet, or squirms in seat.
- Often leaves seat in situations when remaining seated is expected.
- Often runs about or climbs in situations where it is not appropriate. In adolescents or adults, this may be limited to feeling restless.
- Often unable to play or take part in leisure activities quietly.
- Is often "on the go," acting as if "driven by a motor."
- Often talks excessively.
- Often blurts out an answer before a question has been completed.
- Often has trouble waiting their turn.
- Often interrupts or intrudes on others — for example, butts into conversations or games.
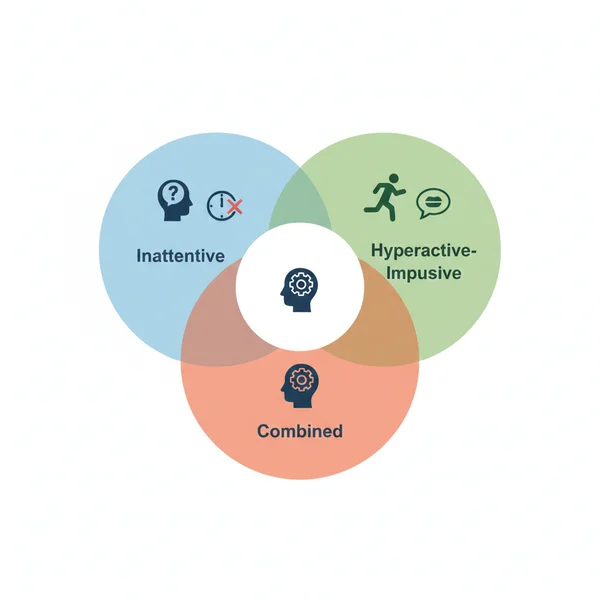
What Are the Three Presentations of ADHD?
The DSM-5 does not describe ADHD as a single condition with one set of symptoms. Instead, it recognizes three distinct presentations based on which symptom category is most prominent.
Predominantly Inattentive Presentation
This presentation applies when someone meets the symptom threshold for inattention but not for hyperactivity-impulsivity. People with this presentation may appear daydreamy, forgetful, or disorganized. They might struggle to stay on task, lose track of conversations, or frequently misplace things. Because these signs tend to be less outwardly disruptive, this presentation is sometimes overlooked — especially in girls and women.
Predominantly Hyperactive-Impulsive Presentation
This presentation applies when someone meets the criteria for hyperactivity-impulsivity but not for inattention. You might notice constant fidgeting, difficulty sitting still, talking excessively, or making impulsive decisions. In younger children, this can look like running or climbing at inappropriate times. In adults, it often shows up as inner restlessness or difficulty relaxing.
Combined Presentation
This is the most commonly diagnosed presentation. It applies when someone meets the symptom threshold for both inattention and hyperactivity-impulsivity. A person with combined presentation may experience difficulty focusing alongside physical restlessness and impulsive tendencies.
It's worth noting that your presentation can change over time. For instance, someone diagnosed with combined presentation in childhood may shift toward predominantly inattentive presentation in adulthood as hyperactive symptoms decrease.
How DSM-5 ADHD Criteria Apply to Adults
One of the most significant updates in the DSM-5 was making ADHD criteria more applicable to adults. Previously, the diagnostic framework was heavily focused on children. Now, the DSM-5 explicitly acknowledges that ADHD can persist into adulthood and adjusts criteria accordingly.
Why the DSM-5 Lowered the Symptom Threshold for Adults
For children up to age 16, the DSM-5 requires six or more symptoms in at least one category. For individuals aged 17 and older, only five symptoms are needed. This adjustment reflects research showing that while ADHD symptoms often continue into adulthood, they may present less obviously. Adults tend to develop coping strategies that can partially mask their difficulties — but that doesn't mean the challenges disappear.
How ADHD Symptoms Often Look Different in Adulthood
In adults, hyperactivity rarely looks like running around a classroom. Instead, it may show up as:
- Feeling internally restless or "wound up"
- Difficulty relaxing or sitting through long meetings
- Constantly shifting between tasks without completing them
- Making impulsive decisions in finances, relationships, or career changes
Inattention in adults might look like chronic lateness, forgetting appointments, struggling with time management, or losing important documents. Because these challenges can overlap with stress or other conditions, many adults go years without recognizing that ADHD may be a factor.
If some of these patterns feel familiar, consider using a structured ADHD self-assessment to organize your observations before discussing them with a healthcare professional.
Key Additional Requirements for an ADHD Diagnosis
Meeting the symptom criteria alone is not enough for a DSM-5 ADHD diagnosis. Several additional conditions must also be satisfied.
Symptoms Must Be Present Before Age 12
The DSM-5 requires that several inattentive or hyperactive-impulsive symptoms were present before the age of 12. This doesn't mean a diagnosis must happen in childhood — rather, looking back, symptoms should have been noticeable by that age. For adults seeking a diagnosis, this often involves recalling childhood experiences or gathering input from family members.
Symptoms Must Appear in Two or More Settings
ADHD symptoms cannot be limited to just one environment. The DSM-5 requires evidence that symptoms are present in at least two settings — such as at home and at school, at home and at work, or with friends and in other activities. This criterion helps distinguish ADHD from situational difficulties.
Functional Impairment and Differential Diagnosis
There must be clear evidence that the symptoms interfere with or reduce the quality of social, academic, or occupational functioning. Additionally, the symptoms should not be better explained by another mental disorder — such as an anxiety disorder, mood disorder, or personality disorder. A trained professional considers all of these factors during evaluation.
What Is the DSM-5 Code for ADHD?
Healthcare providers and insurance companies use specific diagnostic codes to document ADHD. Under the DSM-5, ADHD uses the ICD-10-CM coding system:
| Code | Presentation |
|---|---|
| F90.0 | Predominantly Inattentive Presentation |
| F90.1 | Predominantly Hyperactive-Impulsive Presentation |
| F90.2 | Combined Presentation |
| F90.9 | Unspecified ADHD |
The code F90.9 is used when symptoms are present but don't clearly fit one specific presentation, or when there isn't enough information to determine the exact type. These codes appear on medical records and insurance claims, so understanding them can be helpful if you're navigating the healthcare system.
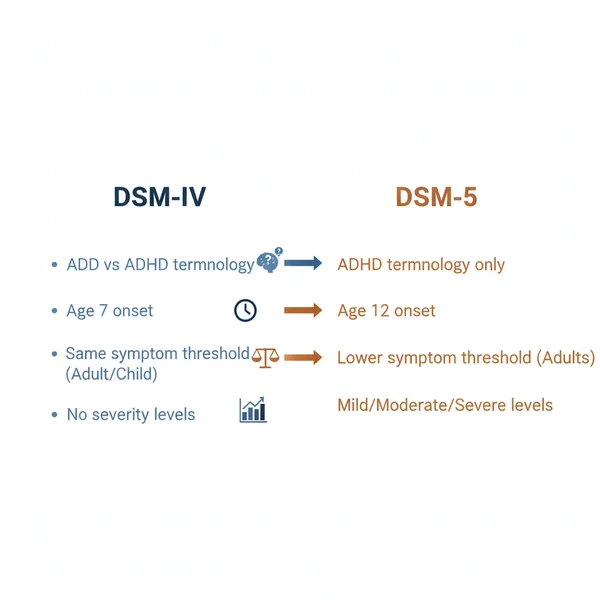
What Changed from DSM-IV to DSM-5 for ADHD?
The DSM-5 introduced several meaningful changes to how ADHD is classified and diagnosed:
- ADD is no longer a separate diagnosis. The DSM-IV used "ADD" (attention deficit disorder) for people with primarily inattentive symptoms. The DSM-5 retired this term and uses only "ADHD" with the three presentations described above.
- Age of onset expanded. The DSM-IV required symptoms to appear before age 7. The DSM-5 changed this to before age 12, recognizing that some individuals — especially those with predominantly inattentive symptoms — may not display noticeable signs until later in childhood.
- Adult symptom threshold lowered. The DSM-5 reduced the required number of symptoms from six to five for individuals aged 17 and older, acknowledging how ADHD manifests differently in adults.
- Severity specifiers added. The DSM-5 introduced mild, moderate, and severe classifications, giving clinicians more flexibility to describe the impact of symptoms on daily life.
- Autism spectrum disorder exclusion removed. The DSM-IV did not allow ADHD to be diagnosed alongside autism spectrum disorder. The DSM-5 permits both diagnoses to coexist.
These changes reflect a more nuanced understanding of ADHD across the lifespan and make the criteria more inclusive for adults and individuals with less obvious presentations.
How to Explore Your ADHD Traits Further
Reading through the DSM-5 ADHD criteria can bring up a range of emotions — from validation to uncertainty. If you recognize yourself in many of these descriptions, that's a meaningful observation worth paying attention to.
This content is for educational purposes only. It is not a clinical diagnosis and should not replace a professional evaluation.
Why Reflecting on Your Patterns Can Be a Helpful First Step
Before scheduling a clinical evaluation, it can help to organize your thoughts. Consider which symptoms you identify with, how long they've been present, and how they affect your daily life across different settings. Writing down specific examples — like trouble meeting deadlines, frequently losing items, or difficulty in conversations — gives you concrete material to share with a professional.
A structured self-reflection tool, like the one at Adhdquiz.net, can guide you through this process. It helps you systematically review patterns related to attention and focus. The goal isn't to arrive at a conclusion — it's to help you understand your experiences more clearly.
When to Consider Talking to a Healthcare Professional
If multiple DSM-5 criteria resonate with your everyday life, and these patterns have been present for a long time across different settings, it may be worth discussing your observations with a qualified professional. This is especially important if your symptoms are affecting your work performance, relationships, or overall well-being.
A professional evaluation typically involves a detailed clinical interview, a review of your history, and sometimes input from people close to you. Only a licensed clinician can make an ADHD diagnosis — but arriving informed and prepared can make the process smoother and more productive.
Key Takeaways on ADHD and the DSM-5
- The DSM-5 is the standard clinical reference for diagnosing ADHD, defining it as a neurodevelopmental disorder.
- There are 18 specific symptoms across two categories: inattention and hyperactivity-impulsivity.
- The DSM-5 recognizes three presentations: predominantly inattentive, predominantly hyperactive-impulsive, and combined.
- Adults need at least five symptoms (rather than six for children) to meet criteria.
- Symptoms must appear before age 12, occur in two or more settings, and cause functional impairment.
- The DSM-5 replaced "ADD" with the unified term "ADHD" and introduced severity specifiers.
Understanding these criteria is a valuable first step toward self-awareness. If you want to reflect on your own attention and focus patterns in a structured way, explore the free ADHD quiz at Adhdquiz.net. Remember, only a licensed professional can provide a formal diagnosis — but being informed helps you take that step with confidence.
Frequently Asked Questions
What is the DSM-5 code for ADHD?
The DSM-5 uses ICD-10-CM codes: F90.0 for predominantly inattentive, F90.1 for predominantly hyperactive-impulsive, F90.2 for combined presentation, and F90.9 for unspecified ADHD. These codes appear on clinical records and insurance documents.
Is ADD still a valid diagnosis under the DSM-5?
No. The DSM-5 replaced "ADD" with "ADHD" as the single unified term. What was previously called ADD now falls under the predominantly inattentive presentation of ADHD.
Can your ADHD presentation change over time?
Yes. ADHD presentations can shift as you age. For example, someone diagnosed with combined presentation in childhood may primarily show inattentive symptoms as an adult, since hyperactive behaviors tend to decrease over time.
What age must symptoms appear by for a DSM-5 ADHD diagnosis?
The DSM-5 requires that several symptoms were present before age 12. This is an expansion from the DSM-IV, which required symptom onset before age 7. Symptoms don't need to have been diagnosed by age 12 — they just need to have been present.
Can adults be diagnosed with ADHD under the DSM-5?
Yes. The DSM-5 explicitly accommodates adult diagnosis by lowering the symptom threshold to five (instead of six for children) and acknowledging that symptoms may look different in adulthood, such as internal restlessness rather than physical hyperactivity.
How many symptoms are needed for an ADHD diagnosis in adults?
Adults aged 17 and older need at least five symptoms of inattention and/or five symptoms of hyperactivity-impulsivity. These symptoms must have been present for at least six months and must cause noticeable difficulty in daily functioning.